Medicare
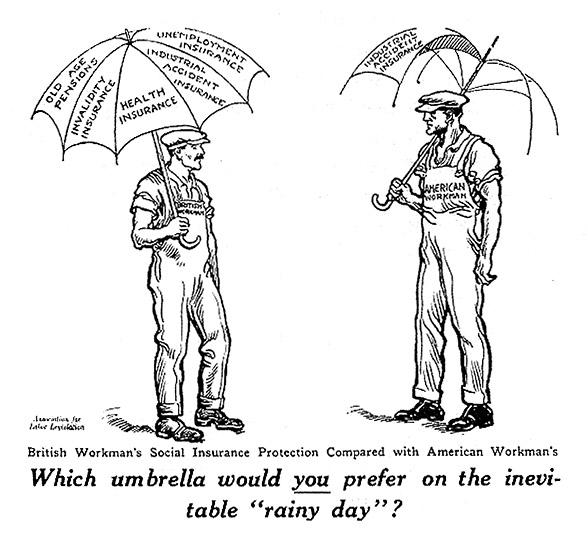
The early 20th century American campaign for protective legislation looked to Germany, England and other European countries which had begun to create safety nets to protect workers and their families from the cycles and crises that came with the modern industrial economy.
Medicare is a national health insurance program enacted in 1965 as an extension of Social Security. It covers up to 80% of hospital, doctor and outpatient costs for persons 65 and older. Like Social Security, Medicare includes insurance programs funded by participants and government-funded supplements to provide for the needy. Part A covers medically necessary hospital, skilled nursing facility, home health and hospice care and is paid for by employee and employer contributions through payroll deductions. These benefits are free if you’ve worked and paid Social Security taxes for at least 10 years. On the other hand, Medicare Parts B, C and D are funded from the annual federal budget in addition to subscriber fees paid by enrollees. Part B covers doctor’s visits, durable medical equipment, outpatient care and home health care. Part C permits private insurance companies (HMO’s and PPO’s) to provide Medicare benefits. Part D is Medicare’s optional prescription drug plan.
The 2010 health care reform legislation (Patient Protection and Affordable Care Act) resulted in significant changes. Part C is now a separate benefit; it permits (and in some cases over-subsidizes) private health insurance companies (through HMOs and PPOs) to provide all Medicare benefits (Parts A, B and D). All too often these private companies insure the healthiest seniors, leaving those in greatest need to Medicare.
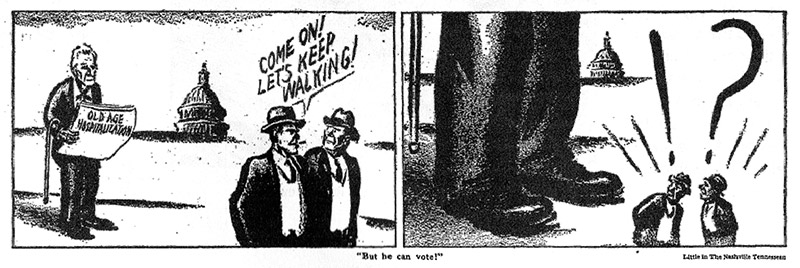
 The AMA mobilized opposition and congressional allies against
Medicare—indeed against any form of national health care
program—again and again, as reformed-minded physicians
advocated for national health care programs.
Herblock, 1938
The AMA mobilized opposition and congressional allies against
Medicare—indeed against any form of national health care
program—again and again, as reformed-minded physicians
advocated for national health care programs.
Herblock, 1938
Medicare is currently under political attack as too costly, even though the Congressional Budget Office recently estimated that it is 11% cheaper than equivalent private insurance plans. The basic insurance plan is not the problem. Longer life expectancy, skyrocketing drug costs and rapidly expanding medical costs within the privatized fee-for-service model of the US healthcare system have resulted in increased costs. Recent federal health care reform legislation imposes a variety of changes on Medicare, including several cost-containment strategies.
Proposals to Change Medicare

Legislators from both parties are debating a range of proposals designed to curb the rising costs of Medicare in the context of maintaining our fee for service system and significantly increased longevity.
Some Republicans propose a Medicare voucher system which would gradually shift Medicare costs from the federal government to senior citizens and local governments (when seniors become impoverished and need Medicaid). The newest Republican proposal (March 2013) would merge Medicare’s hospital and doctor coverage into one program in order to generate savings.
Some Democrats propose maintaining physician reimbursement rates at current levels (to keep doctors in the system); establishing a public insurance option (based on Medicare) to compete with private plans; and aligning Medicare drug payment policies with the more cost-effective Medicaid policies.